


By Yusuf Ahmed, Mostafa Bondok, Patrick Gooi, and R. Rishi Gupta
The Surgical Chair
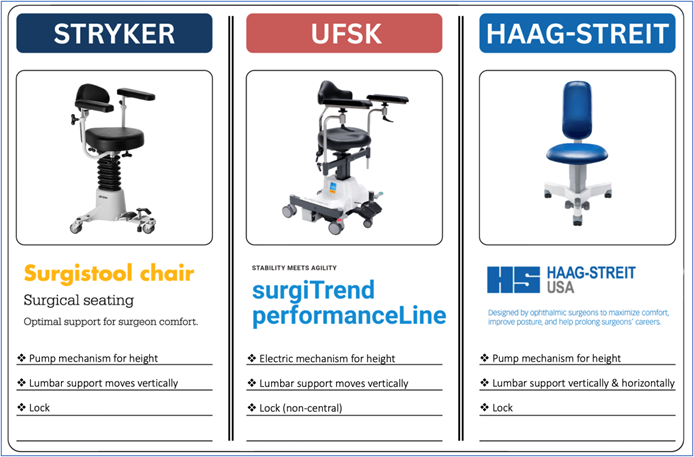
Ergonomic positioning in the OR begins with the surgical chair. Key features to consider include adjustable height (manual or electric), vertically adjustable lumbar support with horizontal adjustability when available, and a locking mechanism that provides stability. Features of commonly used chairs are provided in the images below.
The locking mechanism, when engaged, stabilizes the surgeon and improves fine motor control by allowing relaxation of the core and large stabilizing muscles. However, this same feature can “trap” the surgeon in a suboptimal position. Once alignment is achieved and the chair locked, it is important to recognize that periodic unlocking and micro-adjustments may be necessary as the case progresses and patient positioning shifts.
Optimize and Renew Your Form
Before the case begins, a brief “form check” is advisable. Relax your body, keep your neck neutral, stack your joints, and drop your shoulders down and back. Your back should be supported by the chair’s lumbar support, and your weight evenly distributed along the seat. Position arms and legs in a comfortable, symmetric posture, with pedals at a distance that doesn’t force reaching forward or backward. Finally, aim for hips slightly higher than knees (i.e., just over 90 degrees).
Poor ergonomic habits in the OR rarely reflect neglect. More often, they arise from cognitive load, time pressure, or fatigue. Surgeons may begin a case with excellent alignment, only to find that concentration, difficult anatomy, or prolonged duration gradually erode posture. When possible, distributing complex cases across the surgical schedule may reduce cumulative musculoskeletal strain in addition to cognitive fatigue.
The OR Microscope: A Static Trap
The OR microscope introduces a unique ergonomic challenge. Once the eyes are engaged in the oculars, the body tends to become fixed in position. If alignment is non-optimal, the surgeon may remain locked in a static, non-neutral posture for extended periods. Traditional advice to “sit up straight” is incorrect. Sustaining a rigid, upright posture increases muscular effort and often leads to compensatory strain. A more effective approach is to assess where the eyes would naturally fall if the body were completely relaxed. Any sensation of effort required to maintain ocular alignment should be treated as a signal that adjustments to the microscope, chair, and/or patient positioning should be made.
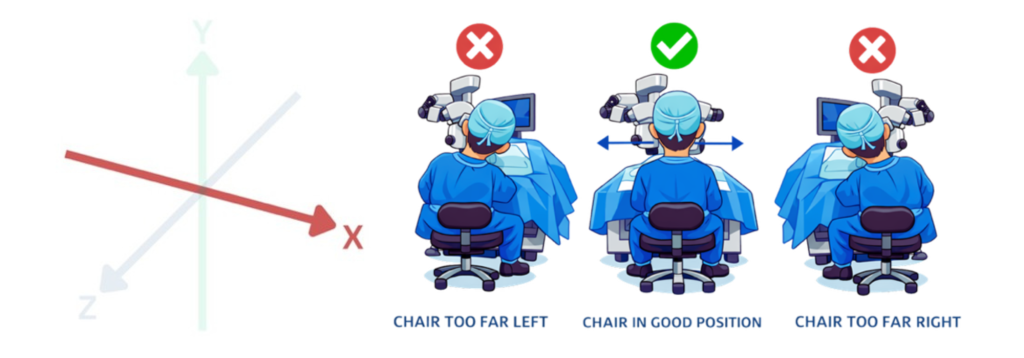
Three-Dimensional Alignment: OR microscope ergonomics can be conceptualized along three axes:
X-axis alignment – refers to left–right positioning. If the microscope is not centred relative to the surgeon, subtle lateral leaning or trunk side-bending occurs. Even small asymmetries can lead to uneven loading of paraspinal muscles and facet joints over time.
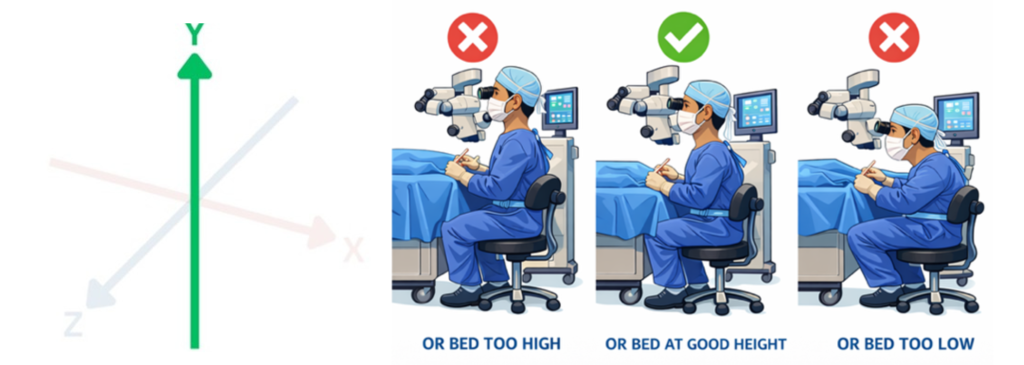
Y-axis alignment – reflects vertical positioning relative to the patient and surgical bed. When seated too low, surgeons compensate with cervical extension, increasing load on posterior cervical elements and paraspinal musculature. When seated too high, forward trunk and neck flexion predominate, increasing anterior cervical disc pressure, upper trapezius strain, and lumbar loading.
Z-axis alignment – refers to forward–backward positioning. Physical constraints imposed by chairs and pedals may prevent surgeons from positioning themselves close enough to the operative field, encouraging forward leaning. This increases lumbar disc pressure and thoracic flexion, often accompanied by compensatory cervical extension. Positioning the patient’s head closer to the edge of the headrest, when safely tolerated, can help reduce the need to reach forward.
