


The OR Microscope – The Danger Zone
By Mostafa Bondok, Patrick Gooi, and R. Rishi Gupta
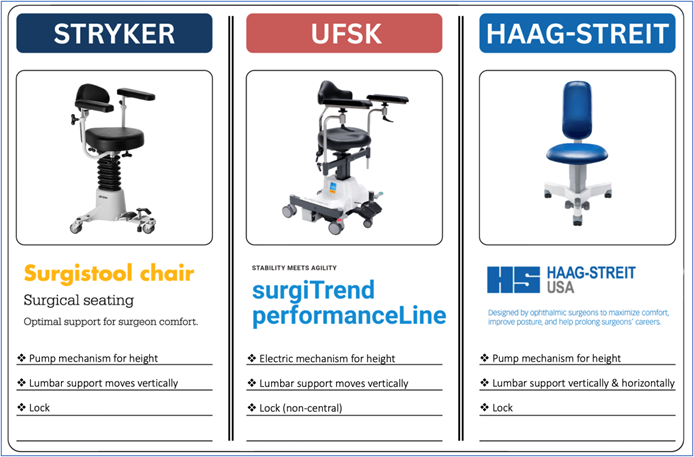
The Surgical Chair
Ergonomic positioning in the OR begins with the surgical chair. Key features to consider include adjustable height (manual or electric), vertically adjustable lumbar support with horizontal adjustability when available, and a locking mechanism that provides stability. Features of commonly used chairs are provided in the images below.
The locking mechanism, when engaged, stabilizes the surgeon and improves fine motor control by allowing relaxation of the core and large stabilizing muscles. However, this same feature can “trap” the surgeon in a suboptimal position. Once alignment is achieved and the chair locked, it is important to recognize that periodic unlocking and micro-adjustments may be necessary as the case progresses and patient positioning shifts.
Optimize and Renew Your Form
Before the case begins, a brief “form check” is advisable. Relax your body, keep your neck neutral, stack your joints, and drop your shoulders down and back. Your back should be supported by the chair’s lumbar support, and your weight evenly distributed along the seat. Position arms and legs in a comfortable, symmetric posture, with pedals at a distance that doesn’t force reaching forward or backward. Finally, aim for hips slightly higher than knees (i.e., just over 90 degrees).
Poor ergonomic habits in the OR rarely reflect neglect. More often, they arise from cognitive load, time pressure, or fatigue. Surgeons may begin a case with excellent alignment, only to find that concentration, difficult anatomy, or prolonged duration gradually erode posture. When possible, distributing complex cases across the surgical schedule may reduce cumulative musculoskeletal strain in addition to cognitive fatigue.
The OR Microscope: A Static Trap
The OR microscope introduces a unique ergonomic challenge. Once the eyes are engaged in the oculars, the body tends to become fixed in position. If alignment is non-optimal, the surgeon may remain locked in a static, non-neutral posture for extended periods. Traditional advice to “sit up straight” is incorrect. Sustaining a rigid, upright posture increases muscular effort and often leads to compensatory strain. A more effective approach is to assess where the eyes would naturally fall if the body were completely relaxed. Any sensation of effort required to maintain ocular alignment should be treated as a signal that adjustments to the microscope, chair, and/or patient positioning should be made.
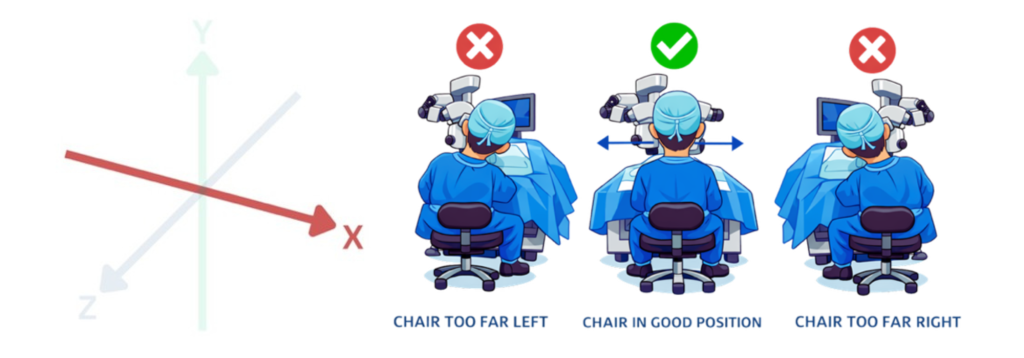
Three-Dimensional Alignment: OR microscope ergonomics can be conceptualized along three axes:
X-axis alignment – refers to left–right positioning. If the microscope is not centred relative to the surgeon, subtle lateral leaning or trunk side-bending occurs. Even small asymmetries can lead to uneven loading of paraspinal muscles and facet joints over time.
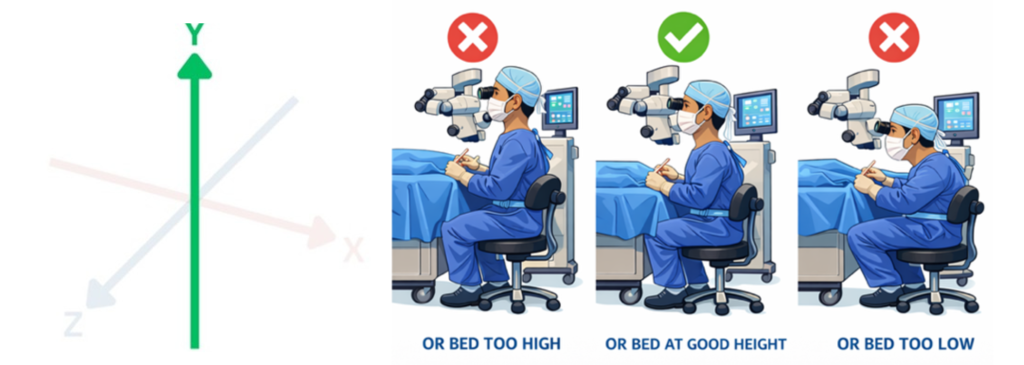
Y-axis alignment – reflects vertical positioning relative to the patient and surgical bed. When seated too low, surgeons compensate with cervical extension, increasing load on posterior cervical elements and paraspinal musculature. When seated too high, forward trunk and neck flexion predominate, increasing anterior cervical disc pressure, upper trapezius strain, and lumbar loading.
Z-axis alignment – refers to forward–backward positioning. Physical constraints imposed by chairs and pedals may prevent surgeons from positioning themselves close enough to the operative field, encouraging forward leaning. This increases lumbar disc pressure and thoracic flexion, often accompanied by compensatory cervical extension. Positioning the patient’s head closer to the edge of the headrest, when safely tolerated, can help reduce the need to reach forward.

Dealing with Physician Burnout
Submitted by: Joshua Huang, University of Alberta
What is Burnout?
According to the World Health Organization, “Burn-out is a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by three dimensions:
- feelings of energy depletion or exhaustion;
- increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job; and
- reduced professional efficacy.” [1]
Epidemiology
Per the Canadian Medical Association’s 2021 National Physician Health Survey [2]:
- More than 50% of attendings and residents report symptoms of burnout
- Increased among general practitioners, remote/rural practitioners, and physicians with fewer years of work experience
- Higher amongst women (59%) vs men (43%)
- >1.5x increase from 2017 results
Risk Factors [3]
- High workload and long hours
- Limited well-being support
- Job dissatisfaction
- Poor sleep hygiene
- Young age (<30 years)
- Personality characteristics such as cynicism, anxiety, difficulty with emotional regulation
- Impersonal and control orientation
Signs & Symptoms [4]
- Physical: Increased heart rate and blood pressure, restlessness, pain, nausea, decreased immune function, frequent headaches
- Affective: Depressed/changing mood, anxiousness, irritability, heightened tension, hypersensitivity, blunted empathy, anger and fear
- Cognitive – Helplessness, cynical perception, pessimism
- Behavioural – emotional outbursts, declined productivity, increased rate of medical errors
- Motivation – decreased motivation, loss of interest, low morale
Treatment
- Individual-level interventions
- Engaging in mindfulness-based therapies, cognitive behavioral therapy, and exercise [5]
- seeking out coaching, writing a gratitude journal, yoga, and building social relationships withpeers and colleagues [6]
- System-level interventions:
- utilizing multidisciplinary team members to lessen physician workload (i.e. documentation, scribes) [6]
- implementing large language models (AI) to help with documentation [6]
References:
- World Health Organization. Burn-out an “occupational phenomenon”: International Classification of Diseases, 2019. May 2019.
- Canadian Medical Association (CMA), Ipsos. CMA 2021 national physician health survey. Ottawa: The Association; 2022 Aug 24
- Shalaby, R., Oluwasina, F., Eboreime, E., El Gindi, H., Agyapong, B., Hrabok, M., … & Agyapong, V. I. O. (2023). Burnout among residents: prevalence and predictors of depersonalization, emotional exhaustion and professional unfulfillment among resident doctors in Canada. International Journal of Environmental Research and Public Health, 20(4), 3677.
- Merlo, G., & Rippe, J. (2021). Physician burnout: A lifestyle medicine perspective. American Journal of Lifestyle Medicine, 15(2), 148-157.
- Antico, L., & Brewer, J. (2025). Digital mindfulness training for burnout reduction in physicians: Clinician-driven approach. JMIR Formative Research, 9(1), e63197.
- Guille, C., & Sen, S. (2024). Burnout, depression, and diminished well-being among physicians. New England Journal of Medicine, 391(16), 1519–1527.
Using the indirect – protect your neck!
Indirect ophthalmoscopy is an essential tool for examination of the peripheral retina. It is a beautifully designed optical instrument for detecting and treating important sight-threatening pathology. However, it is also a physically demanding technique that forces the neck and back into unnatural positions of tilt and hyperflexion. Not only is this strenuous at the time of the exam, but it creates potentially excessive stress on the paraspinal muscles, ligaments, and tendons. Combined with the intense pace of a busy high-volume clinic, it is the perfect recipe for career ending disk herniation, stenosis, or nerve impingement.
In order to reduce the detrimental effects:
- Optimize the patient’s head position by tilting it 30-45 degrees towards you.
- Walk around the patient’s head while examining them to avoid twisting or craning your neck and back. Position your body to remain 180 degrees opposite to the fundus location you are examining, whenever possible.
- Avoid excessive hunching. Keep your neck and back in as neutral a position as possible by elevating the patient’s chair height as high as possible to avoid crouching over.
- Procure yourself a lighter-weight indirect ophthalmoscope in order to reduce the weight on your neck and shoulders.
- Take breaks. This applies especially to learners. If your patient is getting tired and so are you, take a break, begin documenting your findings, have a stretch, and resume.
- Stay fit. A healthy lifestyle and regular exercise, incorporating stretching and strength training, will help keep your joints mobile and more forgiving.
In summary, indirect ophthalmoscopy is challenging enough as it is. Next time you are hunting through vitreous hemorrhage for a retinal tear, please consider incorporating some of these ergonomics tips. Your neck (and the rest of your body) will thank you!
The earlier that proper positioning is adopted and becomes habit, the less likely that potentially career-threatening musculoskeletal injuries will develop.
Michael Dollin, MD, FRCSC
Ergonomics and Injury Prevention Working Group

A Heavy Heart – Globe and Mail
Recommended by Dr. R. Rishi Gupta, this Globe and Mail article offers an important reflection on physician wellness and the physical and mental toll of striving for excellence in medicine. It’s a meaningful read for anyone interested in ergonomics, balance, and sustainable practice.
Ergonomics: Magazine Articles
Title: Ergonomics Simplified
Author: Camille V. Palma, MD
Publisher: EyeNet Magazine
Date: March 2023
Link: https://www.aao.org/eyenet/article/ergonomics-simplified
Title: Ergonomics in Ophthalmology a Lifelong Project
Authors: Alex Young, featuring Nicole Bajic, MD
Publisher: Healio – Ocular Surgery News
Date: December 2022
Link: https://www.healio.com/news/ophthalmology/20221220/ergonomics-in-ophthalmology-a-lifelong-project
Title: The Importance of Ergonomics in the Clinic and OR
Authors: Ellen Stodola, Editorial Co-Director
Publisher: EyeWorld
Date: December 2022
Link: https://www.eyeworld.org/2022/ergonomics-in-the-clinic-and-or/
Title: Ergonomics: Care for Yourself to Improve Patient Care
Author: Peggy Denny, Contributing Writer
Publisher: EyeNet Magazine
Date: August 2022
Link: https://www.aao.org/eyenet/article/ergonomics-care-for-yourself-improve-patient-care?august-2022
Title: Ergonomics In the Clinic and OR
Authors: Deepinder K. Dhaliwal, MD, L.AC; Alison D. Early, MD; Steven G. Safran, MD
Publisher: Glaucoma Today
Date: January/February 2022
Link: https://glaucomatoday.com/articles/2022-jan-feb/ergonomics-in-the-clinic-and-or
Title: Good Posture, Ergonomics and Exercise Key to Long Career for Ophthalmologists
Author: Richard L. Lindstrom, MD
Publisher: Healio – Ocular Surgery News
Date: January 2022
Link: https://www.healio.com/news/ophthalmology/20220105/good-posture-ergonomics-and-exercise-key-to-long-career-for-ophthalmologists
Title: Ergonomic Environment Critical to Well-Being of Eye Specialists
Author: Michela Cimberle
Publisher: Healio – Ocular Surgery News
Date: January 2022
Link: https://www.healio.com/news/ophthalmology/20220105/ergonomic-environment-critical-to-wellbeing-of-eye-specialists
Title: Ergonomics: Perfect Your Posture
Author: Deepinder K. Dhaliwal, MD, L.AC
Publisher: Ophthalmology Management
Date: October 2021
Link: https://digital.ophthalmologymanagement.com/publication/frame.php?i=723043&p=&pn=&ver=html5&view=articleBrowser&article_id=4124260
Title: Making The Retina Workplace More Ergonomically Friendly
Author: Sunir Garg, MD, FACS
Publisher: RETINA SPECIALIST
Date: September/October 2021
Link: https://www.retina-specialist.com/article/making-the-retina-workplace-more-ergonomically-friendly
Title: Ergonomics for the Retinal Physician: Protect Your Musculoskeletal Health with These Tips for Daily Practice
Authors: Megan Nichols, MD; Jeffrey Marx, MD
Publisher: Retinal Physician
Date: May 2019
Link: https://www.retinalphysician.com/issues/2019/may/ergonomics-for-the-retinal-physician/
Title: Ophthalmologists Raise Awareness of Workstyle-Related Ergonomic Problems
Author: Michela Cimberle
Publisher: Healio – Ocular Surgery News
Date: May 2019
Link: https://www.healio.com/news/ophthalmology/20190502/ophthalmologists-raise-awareness-of-workstylerelated-ergonomic-problems
Title: Ergonomics: How Not to Sacrifice Your Body
Author: Liam Jordan, Associate Editor
Publisher: Review of Ophthalmology
Date: October 2018
Link: https://www.reviewofophthalmology.com/article/ergonomics-how-not-to-sacrifice-your-body
Title: Ophthalmic Ergonomics: Continuing Challenges and New Insights
Authors: Linda Roach, Contributing Writer, interviewing Kenneth L. Cohen, MD; Jeffrey L. Marx, MD; Safeer F. Siddicky, MS; Scott E. Olitsky, MD
Publisher: EyeNet Magazine
Date: April 2018
Link: https://www.aao.org/eyenet/article/ophthalmic-ergonomics
Title: Watch Your Back (and Neck and Wrists): Work-related musculoskeletal disorders can shorten your career
Authors: Timothy Ratzlaff, MD; Ashley Brissette, MD, MSc
Publisher: CRSToday
Date: February 2018
Link: https://crstoday.com/articles/2018-feb/watch-your-back-and-neck-and-wrists
Title: Ergonomics, Part Two: Seven Risk Factors and Seven Solutions
Author: Linda Roach, Contributing Writer
Publisher: EyeNet Magazine
Date: November 2014
Link: https://www.aao.org/eyenet/article/ergonomics-part-two-seven-risk-factors-seven-solut
Title: Ergonomics and Retina
Authors: Michael Dollin, MD; with Sunir J. Garg, MD; Sonia Mehta, MD; and Marc Spirn, MD
Publisher: Retina Today
Date: May/June 2014
Link: https://retinatoday.com/articles/2014-may-june/ergonomics-and-retina
Title: Ergonomics, Part Two: Seven Risk Factors and Seven Solutions
Title: Of Ophthalmologists & Aching Backs: With repetitive stress injuries, the doctor becomes the patient. Here’s how to protect your body — and your practice
Author: René Luthe, Senior Associate Editor
Publisher: Ophthalmology Management
Date: January 2012
Link: https://ophthalmologymanagement.com/issues/2012/january/of-ophthalmologists-aching-backs/
Title: Will Ophthalmology Cripple You?
Author: Christopher Kent, Senior Editor
Publisher: Review of Ophthalmology
Date: October 2011
Link: https://www.reviewofophthalmology.com/article/will-ophthalmology-cripple-you
Title: Fellows’ Focus: Ergonomics for the Retina Specialist
Authors: Allen Chiang, MD; Paul S. Baker, MD; Eugene A. Milder, MD; Sunir J. Garg, MD
Publisher: Retina Today
Date: July/August 2010
Link: https://retinatoday.com/articles/2010-july-aug/ergonomics-for-the-retina-specialist
Title: Ergonomics, Part One: Is the Job You Love a Pain in the Neck?
Author: Linda Roach, Contributing Writer
Publisher: EyeNet Magazine
Date: July 2007
Link: https://www.aao.org/eyenet/article/ergonomics-part-one-is-job-you-love-pain-in-neck
Ergonomics: Journal Articles & Editorials
- Aloqab A, Alturkistany W, Ali HMN. The relationship between surgical loupes usage, workplace ergonomics, and musculoskeletal disorders among Saudi ophthalmologists. Saudi Journal of Ophthalmology. 2024; 3;39(2):166-173. DOI: 10.4103/sjopt.sjopt_276_23. https://pubmed.ncbi.nlm.nih.gov/40642356/
- Morrison AK, Kumar S, Amin A, Urban M, Kleinman B. An ergonomic risk assessment of ophthalmology residents using the Rapid Entire Body Assessment (REBA) scale. Cureus 2024;16(2):e53698. DOI: 10.7759/cureus.53698. https://pubmed.ncbi.nlm.nih.gov/38455825/
- Kamei M, Suzuki H, Terayama H, et al. Ergonomic benefit using heads-up display compared to conventional surgical microscope in Japanese ophthalmologists. PLoS One 2024;19(5):e0297461. DOI: 10.1371/journal.pone.0297461. https://pubmed.ncbi.nlm.nih.gov/38776346/
- Barrios EL, Polcz VE, Hensley SE, et al. A narrative review of ergonomic problems, principles, and potential solutions in surgical operations. Surgery 2023;174(2):214-221. DOI: 10.1016/j.surg.2023.04.003. https://pubmed.ncbi.nlm.nih.gov/37202309/
- Fouzdar Jain S, Akhter S, Ishihara R, Siddicky S, High R, Suh DW. The prevalence of work-related musculoskeletal disease among pediatric ophthalmologists. Clinical Ophthalmology 2022;16:833-840. DOI: 10.2147/OPTH.S343155. https://pubmed.ncbi.nlm.nih.gov/35330751/
- Cerier E, Hu A, Goldring A, Rho M, Kulkarni SA. Ergonomics Workshop Improves Musculoskeletal Symptoms in General Surgery Residents. Journal of Surgical Research 2022;280:567-574. DOI: 10.1016/j.jss.2022.06.014.https://pubmed.ncbi.nlm.nih.gov/35787315/
- Albanesi B, Piredda M, Bravi M, et al. Interventions to prevent and reduce work-related musculoskeletal injuries and pain among healthcare professionals. A comprehensive systematic review of the literature. Journal of Safety Research 2022;82:124-143. DOI: 10.1016/j.jsr.2022.05.004. https://pubmed.ncbi.nlm.nih.gov/36031239/
- Aaron KA, Vaughan J, Gupta R, et al.The risk of ergonomic injury across surgical specialties. PLoS One 2021;16(2):e0244868. DOI: 10.1371/journal.pone.0244868. https://pubmed.ncbi.nlm.nih.gov/33561117/
- Schechet SA, DeVience E, DeVience S, Shukla S, Kaleem M. Survey of musculoskeletal disorders among US ophthalmologists. Digital Journal of Ophthalmology 2021;26(4):36-45. DOI: 10.5693/djo.01.2020.02.001. https://pubmed.ncbi.nlm.nih.gov/33867881/
- Koshy K, Syed H, Luckiewicz A, Alsoof D, Koshy G, Harry L. Interventions to improve ergonomics in the operating theatre: A systematic review of ergonomics training and intra-operative microbreaks. Annals of Medicine & Surgery (Lond) 2020;55:135-142. DOI: 10.1016/j.amsu.2020.02.008. https://pubmed.ncbi.nlm.nih.gov/32477512/
- Betsch D, Gjerde H, Lewis D, Tresidder R, Gupta RR. Ergonomics in the operating room: it doesn’t hurt to think about it, but it may hurt not to! Canadian Journal of Ophthalmology 2020;55(3 Suppl 1):17-21. DOI: 10.1016/j.jcjo.2020.04.004. https://pubmed.ncbi.nlm.nih.gov/32448408/
- Weng CY, Hariprasad SM, Leiderman YI. Ergonomics in retina. Ophthalmic Surgery, Lasers and Imaging Retina 2019;50(9):537-542. DOI: 10.3928/23258160-20190905-01. https://pubmed.ncbi.nlm.nih.gov/31589750/
- Epstein S, Tran BN, Capone AC, et al. The current state of surgical ergonomics education in U.S. surgical training: a survey study. Annals of Surgery 2019;269(4):778-784. DOI: 10.1097/SLA.0000000000002592. https://pubmed.ncbi.nlm.nih.gov/29381528/
- Diaconita V, Uhlman K, Mao A, Mather R. Survey of occupational musculoskeletal pain and injury in Canadian ophthalmology. Canadian Journal of Ophthalmology 2019;54(3):314-322. DOI: 10.1016/j.jcjo.2018.06.021. https://pubmed.ncbi.nlm.nih.gov/31109470/
- Bonafede L, Kazmierczak L, Siddicky SF, Gunton KB. Ergonomics in strabismus surgery. Current Opinion in Ophthalmology 2019;30(5):331-336. DOI: 10.1097/ICU.0000000000000594. https://pubmed.ncbi.nlm.nih.gov/31313751/
- Ratzlaff TD, Diesbourg TL, McAllister MJ, von Hacht M, Brissette AR, Bona MD. Evaluating the efficacy of an educational ergonomics module for improving slit lamp positioning in ophthalmology residents. Canadian Journal of Ophthalmology 2019;54(2):159-163. DOI: 10.1016/j.jcjo.2018.05.016. https://pubmed.ncbi.nlm.nih.gov/30975337/
- Kaup S, Shivalli S, Kulkarni U, Arunachalam C. Ergonomic practices and musculoskeletal disorders among ophthalmologists in India: An online appraisal. European Journal of Ophthalmology 2020;30(1):196-200. DOI: 10.1177/1120672118815107. https://pubmed.ncbi.nlm.nih.gov/30474398/
- Venkatesh R, Kumar S. Back pain in ophthalmology: National survey of Indian ophthalmologists. Indian Journal of Ophthalmology 2017;65(8):678-682. DOI: 10.4103/ijo.IJO_344_17. https://pubmed.ncbi.nlm.nih.gov/28820152/
- Shaw C, Bourkiza R, Wickham L, McCarthy I, McKechnie C. Mechanical exposure of ophthalmic surgeons: a quantitative ergonomic evaluation of indirect ophthalmoscopy and slit-lamp biomicroscopy. Canadian Journal of Ophthalmology 2017;52(3):302-307. DOI: 10.1016/j.jcjo.2016.09.011. https://pubmed.ncbi.nlm.nih.gov/28576213/
- 2Honavar SG. Head up, heels down, posture perfect: Ergonomics for an ophthalmologist. Indian Journal of Ophthalmology 2017;65(8):647-650. DOI: 10.4103/ijo.IJO_711_17. https://pubmed.ncbi.nlm.nih.gov/28820146/
- Sivak-Callcott JA, Mancinelli CA, Nimbarte AD. Cervical occupational hazards in ophthalmic plastic surgery. Current Opinion in Ophthalmology 2015;26(5):392-8. DOI: 10.1097/ICU.0000000000000182. https://pubmed.ncbi.nlm.nih.gov/26247136/
- Alrashed WA. Ergonomics and work-related musculoskeletal disorders in ophthalmic practice. Imam Journal of Applied Sciences 2016;1(2):48-63. DOI: 10.4103/ijas.ijas_24_16. https://journals.lww.com/ijas/fulltext/2016/01020/ergonomics_and_work_related_musculoskeletal.2.aspx
- Hyer JN, Lee RM, Chowdhury HR, Smith HB, Dhital A, Khandwala M. National survey of back & neck pain amongst consultant ophthalmologists in the United Kingdom. International Ophthalmology 2015;35(6):769-775. DOI: 10.1007/s10792-015-0036-z. https://pubmed.ncbi.nlm.nih.gov/25609503/
- Herzog NV, Beharic RV, Beharic A, Buchmeister B. Ergonomic analysis and simulation in department of ophthalmology. Procedia Manufacturing 2015;3:128-135. DOI: 10.1016/j.promfg.2015.07.117. https://www.researchgate.net/publication/283960343_Ergonomic_Analysis_and_Simulation_in_Department_of_Ophthalmology
- Fethke NB, Schall MC, Determan EM, Kitzmann AS. Neck and shoulder muscle activity among ophthalmologists during routine clinical examinations. International Journal of Industrial Ergonomics 2015;49:53-59. DOI: 10.1016/j.ergon.2015.06.001. https://www.sciencedirect.com/science/article/abs/pii/S0169814115300019
- Hedge A, James T. Detrimental Effects of an electronic health records system on musculoskeletal symptoms among health professionals. Proceedings of the Human Factors and Ergonomics Society Annual Meeting 2014;58(1):773-777. DOI: 10.1177/1541931214581141. https://www.researchgate.net/publication/271722221_Detrimental_Effects_of_an_Electronic_Health_Records_System_on_Musculoskeletal_Symptoms_among_Health_Professionals#:~:text=Exposure%20to%20blood%20and%20body,of%20health%20practitioners%20surveyed%20reported
- Mehta S, Hubbard GB, 3rd. Avoiding neck strain in vitreoretinal surgery: an ergonomic approach to indirect ophthalmoscopy and laser photocoagulation. Retina 2013;33(2):439-41. DOI: 10.1097/IAE.0b013e318276cbca. https://pubmed.ncbi.nlm.nih.gov/23190927/
- Dorion D, Darveau S. Do micropauses prevent surgeon’s fatigue and loss of accuracy associated with prolonged surgery? An experimental prospective study. Annals of Surgery 2013;257(2):256-9. DOI: 10.1097/SLA.0b013e31825efe87. https://pubmed.ncbi.nlm.nih.gov/22824853/
- Marx JL. Ergonomics: back to the future. Ophthalmology 2012;119(2):211-2. DOI: 10.1016/j.ophtha.2011.09.001. https://pubmed.ncbi.nlm.nih.gov/22305308/
- Kitzmann AS, Fethke NB, Baratz KH, Zimmerman MB, Hackbarth DJ, Gehrs KM. A survey study of musculoskeletal disorders among eye care physicians compared with family medicine physicians. Ophthalmology 2012;119(2):213-20. DOI: 10.1016/j.ophtha.2011.06.034. https://pubmed.ncbi.nlm.nih.gov/21925736/
- Theou O, Soon Z, Filek S, et al. Changing the sheets: a new system to reduce strain during patient repositioning. Nursing Research 2011;60(5):302-8. DOI: 10.1097/NNR.0b013e318225b8aa. https://pubmed.ncbi.nlm.nih.gov/21873921/
- Sivak-Callcott JA, Diaz SR, Ducatman AM, Rosen CL, Nimbarte AD, Sedgeman JA. A survey study of occupational pain and injury in ophthalmic plastic surgeons. Ophthalmic Plastic & Reconstructive Surgery 2011;27(1):28-32. DOI: 10.1097/IOP.0b013e3181e99cc8. https://pubmed.ncbi.nlm.nih.gov/20859236/
- Dhimitri KC, McGwin G Jr., McNeal SF, et al. Symptoms of musculoskeletal disorders in ophthalmologists. American Journal of Ophthalmology 2005;139(1):179-81. DOI: 10.1016/j.ajo.2004.06.091. https://pubmed.ncbi.nlm.nih.gov/15652844/
- Piccoli B, Committee IS. A critical appraisal of current knowledge and future directions of ergophthalmology: consensus document of the ICOH Committee on ‘Work and Vision’. Ergonomics 2003;46(4):384-406. DOI: 10.1080/0014013031000067473. https://pubmed.ncbi.nlm.nih.gov/12637175/
- Wallace RB, 3rd. The 45 degree tilt: improvement in surgical ergonomics. Journal of Cataract & Refractive Surgery 1999;25(2):174-6. DOI: 10.1016/s0886-3350(99)80122-9. https://pubmed.ncbi.nlm.nih.gov/9951660/
- Chatterjee A, Ryan WG, Rosen ES. Back pain in ophthalmologists. Eye (Lond) 1994;8 ( Pt 4):473-4. DOI: 10.1038/eye.1994.112. https://pubmed.ncbi.nlm.nih.gov/7821477/
Can Vitamin D Help with Dry Eyes?
Submitted by: Edmond Sandouk
Overview
Dry eye disease (DED) is a multifactorial disorder of theocular surface, in which inflammation is a central component of both symptoms and pathogenesis[1].
While vitamin D is recognized for its role in calcium regulation and bone health, it also has immunomodulatory and anti-inflammatory properties that may benefit ocular health[2].
Multiple studies have investigated the impact of systemic vitamin D supplementation on DED. Notably, Bae et al. conducted a randomized controlled trial on patients with DED and vitamin D deficiency. They demonstrated significant improvements in tear break-up time (TBUT), Schirmer’s test and ocular surface disease index (OSDI) scores following vitamin D supplementation[3, 4].
Building on this promising evidence, a recent clinical trial led by Hassanpour et al explored a novel approach: topical vitamin D eye drops[5].
Study Title
Safety and Efficacy of Topical Vitamin D in the Management of Dry Eye Disease Associated With Meibomian Gland Dysfunction: A Placebo-Controlled Double-Blind Randomized Controlled Trial[5].
Q&A: Insights from the Study
Q: What was the rationale for testing topical vitamin D?
A: Given the positive ocular benefits of systemic vitamin D, this study aimed to assess whether topical administration could provide local therapeutic effects in patients with DED associated with meibomian gland dysfunction (MGD).
Q: What was the study design?
A: The study was a double-blind randomized control trial including 56 patients with both DED and MGD. They were randomly assigned to receive either vitamin D eye drops or placebo eye drops, administered in one eye four times daily for 8 weeks.
Q: What were the results?
A: At 8 weeks, the vitamin D group demonstrated statistically significant improvements across all major outcomes compared to the placebo group:
- Corneal fluorescein staining: improved ocular surface integrity
- Dry Eye Questionnaire (DEQ 5): reduced subjective symptoms of dry eyes
- Schirmer test: increased tear production
- TBUT: longer tear film breakup time
- Meibomian gland expressibility score: improved gland function
- OSDI score: reduced severity of DED
Q: Were there any adverse effects?
A: The treatment was well tolerated. There were no statistically significant ocular adverse events compared to the placebo group, and no participants discontinued the study due to side effects.
Q: Are topical vitamin D eye drops commercially available?
A: The eye drops were specifically prepared for research purposes and are not currently available on the market.
Conclusion
Topical vitamin D appears to be a safe and promising option for the treatment of DED associated with MGD. This study highlights the need for further research and development of vitamin D-based ocular therapies.
References
1. Clayton, J.A., Dry Eye. N Engl J Med, 2018. 378(23): p. 2212-2223.
2. Sassi, F., C. Tamone, and P. D’Amelio, Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients, 2018. 10(11).
3. Bae, S.H., et al., Vitamin D Supplementation for Patients with Dry Eye Syndrome Refractory to Conventional Treatment. Sci Rep, 2016. 6: p. 33083.
4. Rolando, M. and S. Barabino, Dry Eye Disease: What Is the Role of Vitamin D? Int J Mol Sci, 2023. 24(2).
5. Hassanpour, K., et al., Safety and Efficacy of Topical Vitamin D in the Management of Dry Eye Disease Associated With Meibomian Gland Dysfunction: A Placebo-Controlled Double-Blind Randomized Controlled Trial. Cornea, 2024. 43(5): p. 552-563.
COS Ergonomics and Injury Prevention Working Group
The Canadian Ophthalmological Society (COS) Ergonomics and Injury Prevention Working Group is committed to promoting physical wellness across all stages of ophthalmology practice. Through educational initiatives, resource development, and collaborative research, we aim to make a focus on ergonomics a standard in Canadian ophthalmic care.
Our Mission: To eliminate work-related injuries for Canadian ophthalmologists.
Our Vision: To educate every Canadian ophthalmologist on ergonomics and how best to mitigate risks.
Our Values: Respect, passion, teamwork, creativity, inclusion, and diversity.
Our Current Projects:
- Canadian Handbook for Ergonomics and Injury Prevention for Ophthalmologists
- Ergonomics Toolbox for Residents
- Resident Ergonomics Curriculum Development
- Social Media Educational Initiatives and Challenges
- Sightlines Ergonomics Educational Initiatives
- SAP: Ergonomics: Doesn’t Hurt To Think About It, But It May Hurt Not To! (Royal College MOC Section 3 Accredited)
- Webinar: We’ve Got Your Back! A COS Working Group in Ergonomics and Injury Prevention Webinar (October 2025)
- Ergonomics Podcast (Fall 2025)
- And many more…!
Ergonomics and Injury Prevention Working Group Members

Journal Articles & Editorials:
Explore the growing body of peer-reviewed research on ergonomics in ophthalmology and microsurgery.
LEARN MORE →

Magazine Articles:
Hear directly from ophthalmologists about real-world experiences, preventive tips, and system-wide challenges related to MSK injury.
LEARN MORE →

Podcasts & Videos:
Prefer to learn on the go? Explore expert-led podcasts and video content on ergonomics in ophthalmology and surgery.
LEARN MORE →

Ophthalmology Educational Series:
Engage with HIGH-YIELD accredited modules and curated training developed by national experts.
LEARN MORE →

Other Ergonomics Resources for Physicians:
Ergonomic challenges affect all healthcare providers. Learn from a broader body of literature in medicine and surgery.
LEARN MORE →
Benign or Malignant? A Introductory Guide to Eyelid Lesions in the Primary Care Setting
Authors and Affiliations:
Mostafa Bondok, MD1; Anne Xuan-Lan Nguyen, MDCM2; Edsel Ing MD, PhD, MBA, MEd, MPH3,2
1: Section of Ophthalmology, Department of Surgery, Cumming School of Medicine, University of Calgary, Calgary, Canada
2: Department of Ophthalmology and Vision Sciences, University of Toronto Temerty School of Medicine, Toronto, Canada
3: Department of Ophthalmology and Visual Sciences, University of Alberta, Edmonton, Canada
Corresponding Author
Edsel Ing MD PhD FRCSC MEd MPH MIAD MBA
Professor & Chair of the Department of Ophthalmology & Visual Sciences
Chief of Ophthalmology Edmonton Zone
10240 Kingsway Avenue, Royal Alexandra Hospital, Edmonton, Alberta, T5H 3V9
(c): 780-735-8784; (e): [email protected]
Funding Statement: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Authors’ Competing Interests: The authors indicate no financial support or conflicts of interest. The authors have no proprietary or commercial interest in any materials discussed in this article. All authors attest that they meet the current ICMJE criteria for authorship.
Eyelid lesions are common in primary care
Most eyelid lesions are benign, but 5-10% of skin cancers are periocular, with 90% being basal cell carcinoma (BCC) and 5% squamous cell carcinoma (SCC) [1]. Risk factors include age, UV exposure, family history, immunosuppression, and fair skin [1]. Sebaceous carcinoma, malignant melanoma and Merkel cell carcinoma are important but less common eyelid malignancies.
Recognition and clinical evaluation of malignant eyelid lesions is crucial
BCC and SCC often affect the lower eyelid or medial canthus due to sun exposure. Evert the eyelids to evaluate the palpebral conjunctiva and fornix and assess for tissue fixation [1]. Features of malignancy include skin ulceration, telangiectasia, loss of eyelashes, distortion of eyelid architecture, and crusting [1,2]. Assess ocular motility, palpate regional lymph nodes, and scan sun-exposed areas on the face and body for other lesions. Unilateral blepharitis, or recurrent chalazia may masquerade as sebaceous carcinoma. The “ABCDE” criteria (Asymmetry, Border irregularity, Colour variation, Diameter >6mm, Evolution) aids in the evaluation of eyelid malignant melanoma.
Refer lesions with malignant features
Malignant lesions can resemble benign ones, making diagnosis challenging [1]. Refer suspicious cases to an oculoplastic surgeon or dermatologist for biopsy [1,2]. Treatment typically involves surgical excision with clear margins via Mohs or frozen section. For inoperable BCC, vismodegib is an option for extensive disease, while imiquimod may treat superficial cases.
Styes and chalazia are frequent in primary care
Generally, a stye is a painful, red, and pimple-like lesion caused by infection [3], whereas a chalazion is a non-infectious, painless bump on the eyelid [2,4]. Both often resolve with warm compresses (5-10 min, 4-5x/day) and lid massage. Persistent cases (>4-6 weeks) warrant referral to ophthalmology for assessment of comorbid eye conditions (e.g., rosacea keratitis, blepharitis) [4], and possible definitive management with antibiotics, steroids, and/or incision & curettage [3,5]. Good eyelid hygiene, including lid scrubs with baby shampoo, aids prevention [3–5].
Other common benign eyelid lesions include epidermal inclusion cysts, hidrocystomas, seborrheic keratoses and nevi
Cystic, non-ulcerated lesions that transilluminate may be sweat duct cysts (hidrocystomas), while non-transilluminating cysts may be epidermal inclusion cysts. Seborrheic keratoses appear greasy and “stuck on,” with variable pigmentation. Eyelid nevi may have little to no pigmentation, and the presence of protruding hairs is not uncommon.
[1] Cook BE, Bartley GB. Treatment options and future prospects for the management of eyelid malignancies: An evidence-based update. Ophthalmology 2001;108:2088–98. https://doi.org/10.1016/S0161-6420(01)00796-5.
[2] Bernardini FP. Management of malignant and benign eyelid lesions. Curr Opin Ophthalmol 2006;17:480–4. https://doi.org/10.1097/01.ICU.0000243022.20499.90.
[3] Lindsley K, Nichols JJ, Dickersin K. Non-surgical interventions for acute internal hordeolum. Cochrane Database of Systematic Reviews 2017;2017. https://doi.org/10.1002/14651858.CD007742.PUB4/MEDIA/CDSR/CD007742/IMAGE_N/NCD007742-AFIG-FIG01.PNG.
[4] Zhu Y, Zhao H, Huang X, Lin L, Huo Y, Qin Z, et al. Novel treatment of chalazion using light-guided-tip intense pulsed light. Sci Rep 2023;13:1–11. https://doi.org/10.1038/s41598-023-39332-x.
[5] Ben Simon GJ, Huang L, Nakra T, Schwarcz RM, McCann JD, Goldberg RA. Intralesional Triamcinolone Acetonide Injection for Primary and Recurrent Chalazia: Is It Really Effective? Ophthalmology 2005;112:913–7. https://doi.org/10.1016/J.OPHTHA.2004.11.037.